Breast Explant Surgery in Tulsa, OK
Posted January 13, 2020 in Uncategorized
Partial vs Total Capsulectomy
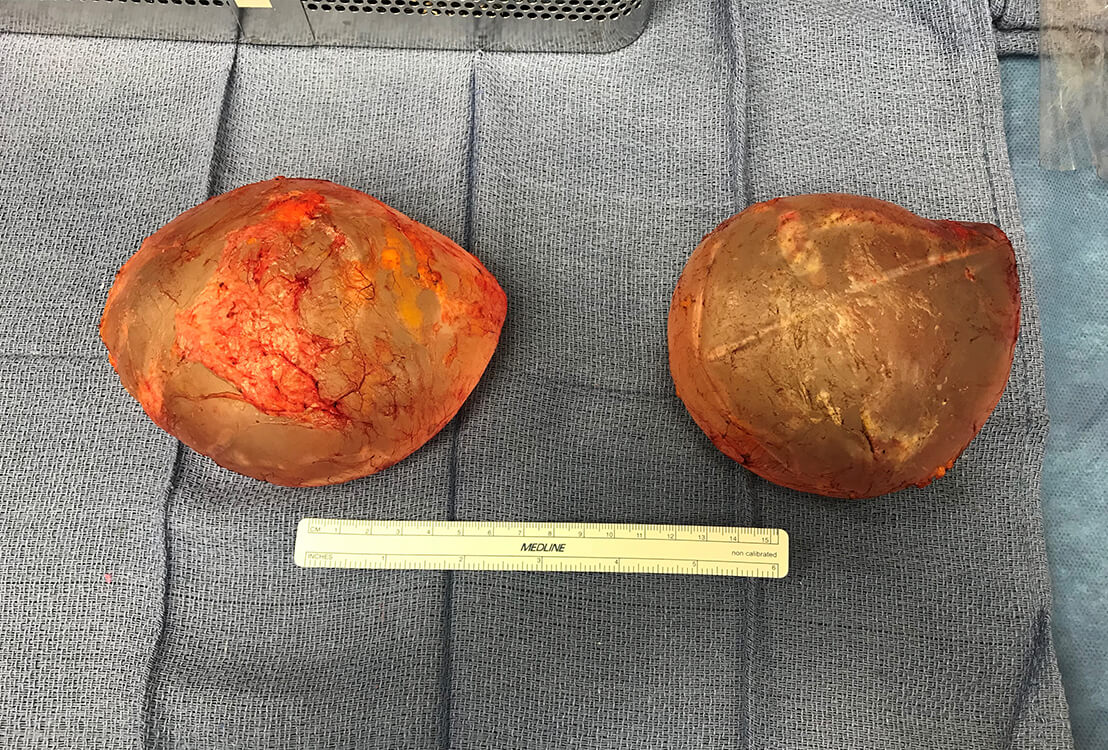
It is always recommended to remove as much of the the capsules as possible when doing an explant. There are several reasons for this which I’ll explain …
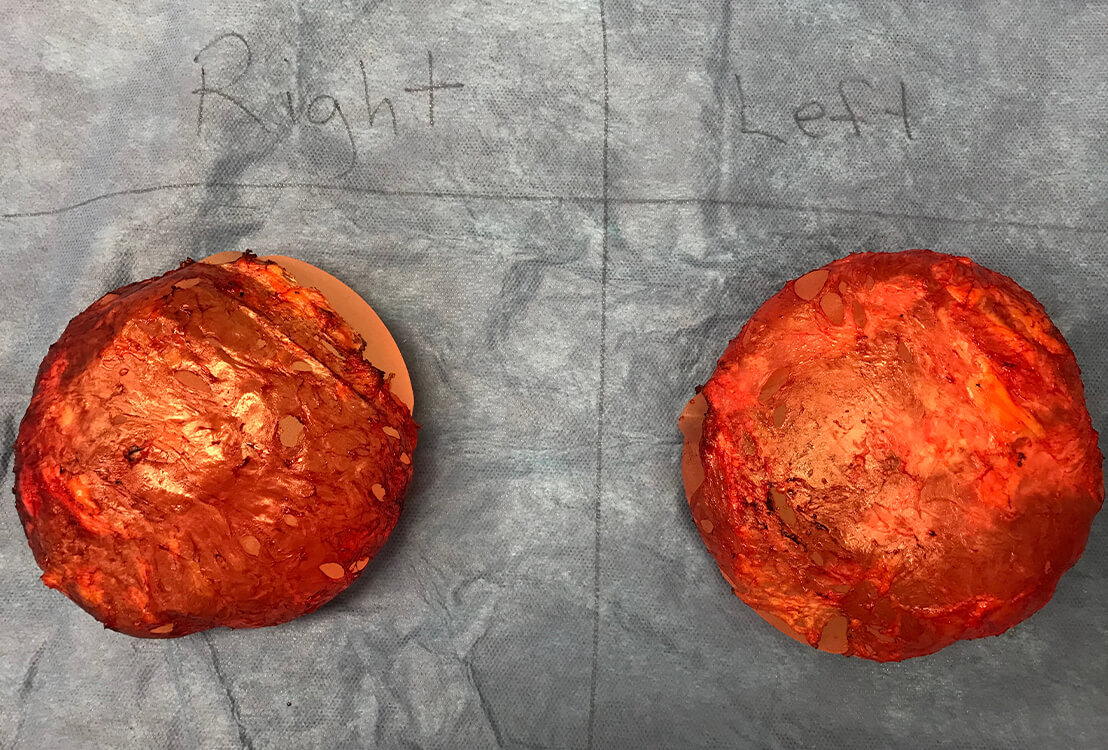
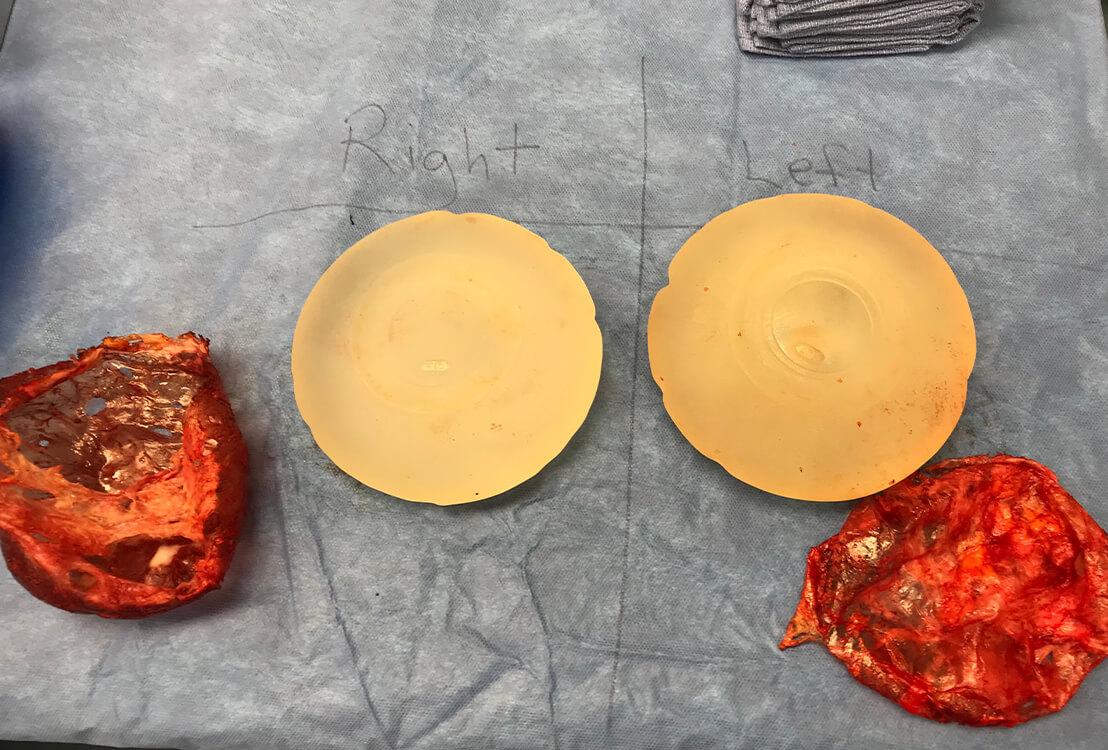
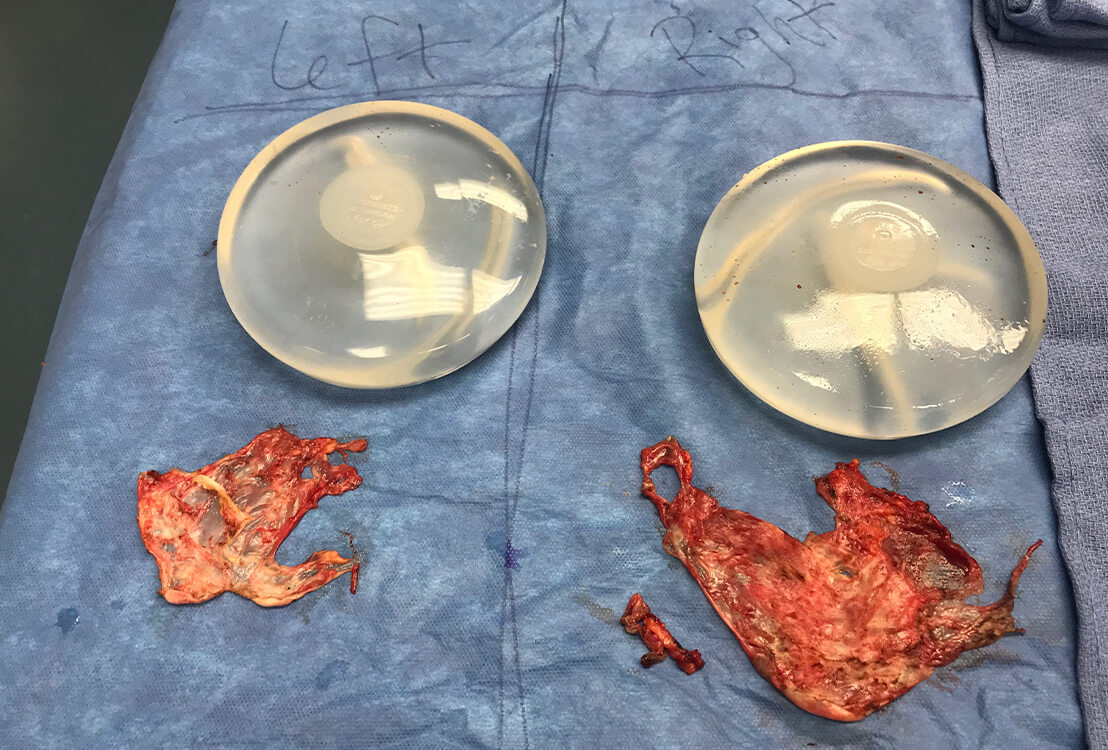
However, it’s not always possible to remove all of the capsule given factors such as capsule thickness and adherence to adjacent tissue. If the capsule is more like a thin film which cannot be separated from the tissue it’s adherent to (such as the pectorals muscle or the ribs), then it is not only impossible to remove it intact, but it is not advisable to put the patient at risk of excessive (possibly uncontrollable) bleeding. The remaining capsule can be cauterized and, of course, the pocket is well irrigated to wash out any “toxins”. It may be possible to remove the capsule “en bloc” or depending on the anatomy and exposure permitted by the approach and patient anatomy, the dissection may occur with the implant in place & then after the implant is removed additional dissection is performed and total or near total capsulectomy achieved … this is no different than en bloc as far as result is concerned. The only time en bloc can be advantageous is in the case of a ruptured silicone implant given the mess they create!
Removal of the capsule is important because studies have shown improved outcome with its removal vs leaving it in …. I do not believe partial vs full capsulectomy was distinguished … but leaving the capsule in entirely and only removing the implant is not appropriate treatment. The capsule needs to be removed and/or cauterized to encourage the pocket to close/scar down. Placing a drain within the pocket also is necessary for this process because the fluid needs to be removed so the 2 sides will adhere to one another and obliterate the space in which the implant used to sit. If the pocket is full of fluid the 2 sides won’t adhere and a potential space will remain … which may stay filled with fluid and potentially be a site for infection….
Remember the capsule is made by the patient … it walls off the implant (foreign body)… various factors are involved in determining capsule thickness … all of which we do not fully understand … as we do not know exactly why some women develop capsular contracture and others do not . In thin patients with very little breast tissue, after implant removal it would be possible to feel a capsule that is thick and/or firm … this of course isn’t desirable.